
01/10/2025
Alex Lyakhovich
Sabancı University Faculty of Engineering and Natural Sciences Faculty Member
Every intro lecture in the "Biology of Aging" course begins with a survey, and my very first question to students is: what is aging and when does it start?
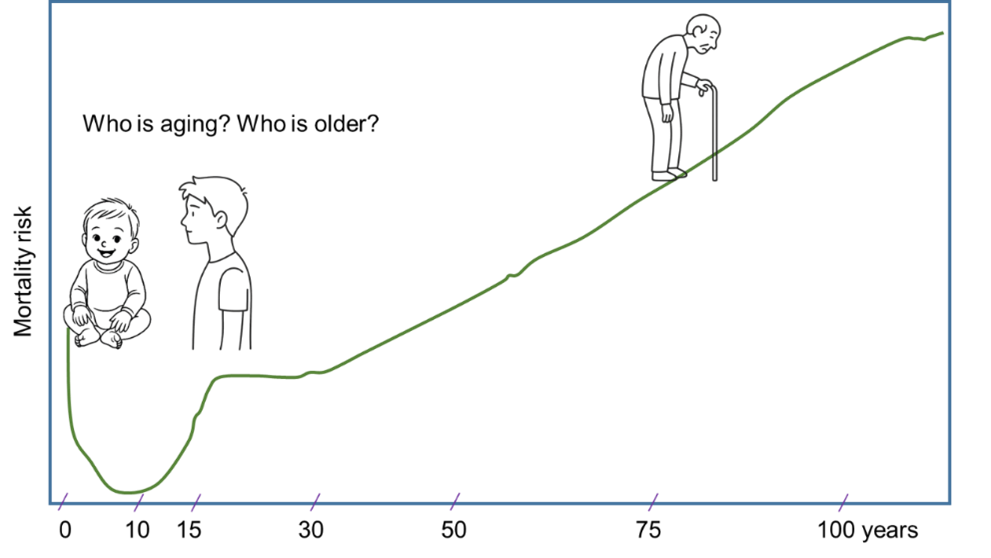
Over the years, I've accumulated dozens of different answers and noticed that none of them are incorrect. But neither is a single correct one. This is because we still don't understand aging, and no universal theory has been developed that would comprehensively explain this process from an evolutionary perspective. For those working in the humanities, I often say that aging is the process of getting old. For those in the natural sciences, I introduce the concept of error accumulation in complex, degenerative biological systems associated with death. However, do not get confused — aging and mortality are two different phenomena. For instance, if we look at the Gompertz curve (the probability of death as a function of age), we see that a child a few months old and a kid 12–15 years old have the same probability of dying. Intuitively, we understand that they have not aged equally. Another word, mortality rates at different ages may be similar in magnitude, but their qualitative nature is completely different. Can this be seen as a "vicious cycle of aging and disease"? To some degree, yes.
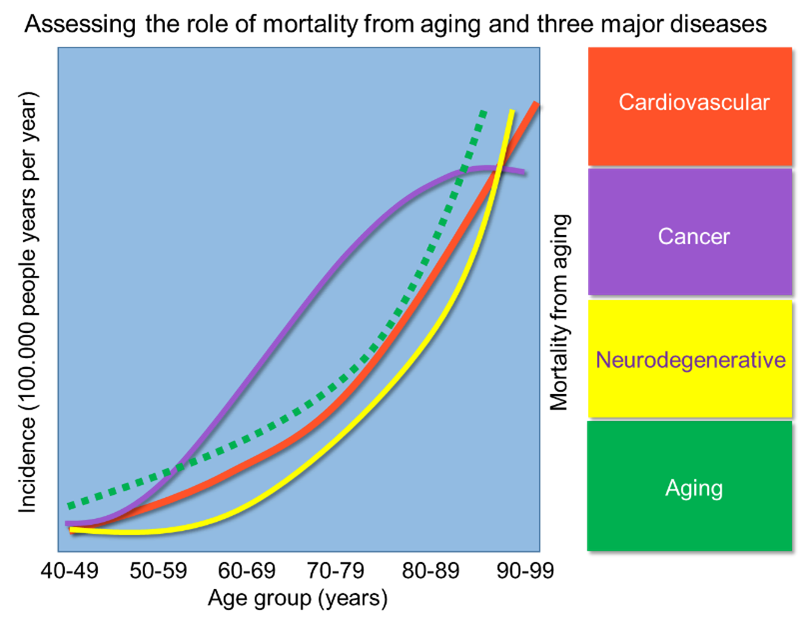
People most often die from three main pathologies: cardiovascular disease, cancer, and neurodegenerative diseases. This triad increases exponentially with age, similar to how our likelihood of death increases after 30-40 years (take a look at a few simple graphs).
Some believe that these pathologies, developing into chronic diseases (inflammation, sarcopenia, cognitive decline), create a state resembling aging. Others think that aging is a primary process of accumulation of damaged biopolymers, decreased regeneration, and weakened immunity, and that diseases are a consequence of general "wear and tear." This question may seem rhetorical, but it is not. If aging is simply a consequence of these diseases, then effectively treating this triad is necessary to live longer (although this will likely only push the cause of death to the next disease). If aging is at the forefront of this triad, then there is no point in curing each disease separately. Simply treat aging, and then cancer, Alzheimer's, or heart failure will automatically recede. But then we must admit that aging is a disease. This is precisely the path the WHO is currently taking, replacing the obscure senility/old age (code R54) in its cause of death registry with XT9T—diseases associated with aging. Perhaps the time has come to lobby insurance companies to invest in aging treatments and provide people with paid aging-related leave, similar to sick leave.
I still doubt this is realistic, but if we're serious about not only equating aging with disease but also trying to cure it, we must learn to measure aging and show how our chronological age, as recorded in our passports, differs from our actual biological age. The most popular approach these days is the epigenetic clock, which correlates patterns of modified DNA residues with an organism's chronological age. The good news is that this clock is ticking. The sad news is that we don't understand how it works. Like the saga of the human genome, we've learned to read the letter sequences of our great bestseller, the DNA book, but we still have a very poor understanding of its meaning. The second problem is that such clocks are quite expensive and extremely imprecise. But why should we care about accuracy? This is truly crucial: if we can improve the accuracy to days or hours, we'll be able to conduct clinical trials of anti-aging drugs in humans, since we won't have to wait years to see if aging has slowed. Incidentally, among other projects in our lab, we are trying to find cheaper and simpler biomarkers of aging, for example, through mitochondria—the organelles responsible for energy production and cellular respiration, whose decline in activity can reflect the biological age of certain organs. Ideally, it would be possible to create universal markers that would predict the expiration dates of organs for replacement. However, when it comes to the large biological clock that predicts a person's own expiration date, we are entering an ethically slippery slope - do we even want to know about it?
So, the biology of aging is one of the extraordinary disciplines undergoing a renaissance in our decade. Among the questions we would like to address in the near future are both fundamental and practical. For fundamental ones, we must ask ourselves: why did aging arise? Single-celled organisms practically never age. But even in multicellular organisms, we now know many examples of ageless (do not mix them with immortal!) animals and plants – from the Hydra vulgaris and the Turritopsis dohrnii jellyfish, to the Greenland shark, the naked mole rat, and even the Bristlecone pines. Why couldn't humans evolve along this path? Why has the maximum lifespan of our species stalled at 122 years, and can we overcome this genetically? Among the practical issues that need to be addressed is the search for aging and longevity genes in humans. Do we have them, and how many are there? Genetic manipulations of animal models have revealed genes that increase lifespan by 30-70%. But it seems that humans are designed differently, and we should think about personalized life extension, shifting the emphasis from maximum lifespan to a “healthy lifespan” that will help avoid age-related diseases. And then the crucial question returns us to where we started: is aging a disease? If so, then it can and should be treated.



